Foot/heel/Achilles issues have given me trouble over the years. The same issues are the scourge of many a runner. Plantar Fasciitis, Achilles tendon pain and metatarsalgia are a few of the problems one can experience as a result of faulty foot and lower-leg mechanics.
The causes of these injuries are often multi-faceted and thus are the solution(s). It seems that weakness of the foot muscles may be a prominent issue. One idea on the mechanism of plantar fasciitis is that the intrinsic foot muscles do a poor job of controlling forces going through the foot. If the stresses of running and walking aren’t distributed adequately then we may overstress the plantar fascia and that may trigger pain. We then need to find a way to unload the stressed tissues. (Please note that this may or may not be what causes plantar fasciitis. There are a lot of questions on how this and other lower-limb pain develops. This study discusses the poor understanding of plantar fasciitis and the difficulty in measuring foot mechanics.) If weak and underperforming foot muscles are part of the problem then how do we bring them back on line?
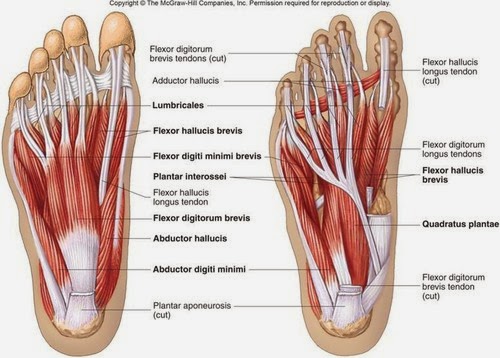
Lots of muscles and joints in those feet.
Among many strategies to address foot pain is an exercise known as the short-foot exercise or foot doming. As the name implies, this exercise has you using the intrinsic foot muscles to create a dome by pulling the metatarsal heads (balls of the toes) toward the heel, which shortens the length of the foot.
The short-foot or foot dome exercise.
More than anything this is a brain exercise. Chances are that when you first try this exercise you won’t do it very well. You’ll struggle, steam may come out of your ears and you’ll get frustrated. Don’t be a baby and give up immediately though. This is a new skill and it takes focused attention and time to develop skills. Keep at it. It likely won’t take you very long to figure it out. For me, the challenge of mastering this exercise is nothing compared to the frustration of being sidelined by foot pain.
Also, try the exercise on your non-hurting foot. If you’re like me, you’ll find that it’s easier to do which again may be an indicator that the source of your pain are muscles that aren’t doing their job correctly.
You may experience cramping. That’s fine. It means you’re doing the exercise correctly. You can either relax the foot muscles and try again or do what I’ve done and hold the short foot until the cramping passes. It hurts a bit but I’ve found the pain to pass quickly.
The muscles involved in this exercise aren’t given to being big and strong. We need them to work a lot for a long time, so we need to condition their endurance. Therefore we need to hold the short foot position for time and we need to do the exercise often throughout the day. The good thing is you need no equipment to do this and you can do it anywhere. You don’t have to take off your shoes either.
I think this video does a good job of describing the exercise:
The last couple of blog posts have shown some hip mobility drills. As the title implies this is about the shoulders and T-spine. There is a lot of motion available in this area and this collection of drills does a fairly good job of getting to a lot of that motion. This is not the be-all-end-all of shoulder/spine mobility work. There are plenty of other shoulder and spine drills in the world That said, these movements have helped me move and feel better and I think they’ve done the same for several of my clients. Here it is:
Cat/Camel
If the T-spine can’t move well then it’s likely that the shoulders won’t move well either. This is a good place to start to get things moving. This yoga exercise usually feels very good, rarely induces pain and it’s easy to do. First I do the original version that has the spine flexing and extending in the saggital plane. I follow that by a side-flexion type of cat/camel. (And to add authenticity, I included an actual cat. Couldn’t get my hands on a camel though.)
3D shoulder mobility
As you can see, all of these are done prone. You can put your arms on a wall and do them standing. There’s also quite a bit of ab work that happens while doing these so you may need to rest between drills.
I’m a fan of mobility. I put a premium on my clients and I having a large “movement database.” I’m not just talking about flexibility mind you. On that note, I like Dr. Andreo Spina’s words on mobility vs flexibility:
“By my definition, mobility and stability are intimately related. Mobility, which is often confused with ‘flexibility,’ can be defined simply as the ability to move or to be moved freely and easily. Another way to think of it is the ability to actively achieve range of motion. Flexibility by contrast is the ability to passively achieve range of motion. It is therefore possible to be very flexible, however have limited mobility. The former implies that you can passively achieve a particular range, while the latter implies neurological control of a particular range as it is being actively attained.”
I’m also very interested in the concept of movement variability. What is “movement variability?” Todd Hargrove of Bettermovement.org discusses it as such:
“Good movement is not just about harmonious interaction or coordination between the different parts of the body. It is most fundamentally about how the system interacts with the environment, particularly in response to unexpected changes. In other words, good movement implies a quality of adaptability and responsiveness to a changing environment.
One can imagine building a humanoid robot that can walk with flawless symmetry and grace. But if the robot cannot adapt its gait pattern to accommodate changes in the terrain, it will fall each time it steps on a rock, and its movement skill is essentially useless. True movement intelligence therefore doesn’t exist so much in the movements themselves, but in their interaction with the environment.
The graceful stride of the deer isn’t useful unless it can be modulated to jump a log and avoid a wolf. A soccer player who can execute technically brilliant ball handling skills in solo practice does not face the real test until she performs those moves in a game situation against an opponent who is trying to steal the ball.
We would not say that someone is fluent in a language if they have only one way to communicate a particular thought, regardless of how perfect that particular communication is. Similarly, one is not fluent in the language of movement unless he can accomplish the same goal in many different ways.”
Why do I mention movement variability? My last blog post was about hip mobility and in it were several different hip mobility drills. This post is also about hip mobility and it features a bunch of different drills. Which ones are best? Who knows? With regard to movement variability, I think it’s probably a good idea to do a lot of different mobility drills and frequently experience novel movement.
Recently I discovered GMB.io. (Yes you read that right.) I’m not sure what GMB stands for but I have enjoyed looking through their content which is very much mobility-centric. Their 8-exercise hip mobility sequence (below) is great! I’ve been using myself and with my clients. Lately I’ve been alternating between this series and the series in the prior post.
I’ve been using the following drills with a lot of my clients as well as with myself. Is this the be-all-end-all collection of hip mobility exercises? Probably not, but I think it hits several nails on the head in terms of movement that’s available to the hips. I think these drills may be especially useful for cyclists and those who are desk-bound. (I’ll be very honest and tell you that I’ve stolen these moves from both Gary Gray and Andreo Spina.) I do them in the order presented but for no other reason than that’s how I do it. You could do any of these in any order.
I use these with most of my clients a lot of the time. I personally use them after a bike ride or long trips in the car or on a plane.
Dean Ornish, MD is a very bright guy. He is the founder and president of the nonprofit Preventive Medicine Research Institute in Sausalito, Calif. He is a professor of medicine at the University of California, San Francisco. He received his medical training in internal medicine from the Baylor College of Medicine, Harvard Medical School, and the Massachusetts General Hospital. He received a BA in humanities summa cum laude from the University of Texas in Austin.
Ornish insists that a very low-fat, high-carb vegetarian diet is the best way to good health. The problem is, he cites low-quality studies and draws conclusions that aren’t quite supported by the available evidence. The article states:
“Ornish goes to argue that protein and saturated fat increase the risk of mortality and chronic disease. As evidence for these causal claims, he cites a handful of observational studies. He should know better. These types of studies—which might report that people who eat a lot of animal protein tend to develop higher rates of disease—“only look at association, not causation,” explains Christopher Gardner, a nutrition scientist at the Stanford Prevention Research Center. They should not be used to make claims about cause and effect; doing so is considered by nutrition scientists to be “inappropriate” and “misleading.” The reason: People who eat a lot of animal protein often make other lifestyle choices that increase their disease risk, and although researchers try to make statistical adjustments to control for these ‘confounding variables,’ as they’re called, it’s a very imperfect science. Other large observational studies have found that diets high in fat and protein are not associated with disease and may even protect against it. The point is, it’s possible to cherry-pick observational studies to support almost any nutritional argument.”
And:
“The recent multicenter PREDIMED trial also supports the notion that fat can be good rather than bad. It found that individuals assigned to eat high-fat (41 percent calories from fat), Mediterranean-style diets for nearly five years were about 30 percent less likely to experience serious heart-related problems compared with individuals who were told to avoid fat. (All groups consumed about the same amount of protein.) Protein, too, doesn’t look so evil when one considers the 2010 trial published in The New England Journal of Medicine that found individuals who had recently lost weight were more likely to keep it off if they ate more protein, along with the 2005 OmniHeart trial that reported individuals who substituted either protein or monounsaturated fat for some of their carbohydrates reduced their cardiovascular risk factors compared with individuals who did not.”
Also, regarding Dean Ornish’s research:
“So there’s little evidence to suggest that we need to avoid protein and fat. But what about the claims Ornish makes about the success of his own diet—do they hold up to scrutiny? Not exactly. His famous 1990 Lifestyle Heart trial involved a total of 48 patients with heart disease. Twenty-eight were assigned to his low-fat, plant-based diet and 20 were given usual cardiac care. After one year those following his diet were more likely to see a regression in their atherosclerosis.
But here’s the thing: The patients who followed his diet also quit smoking, started exercising and attended stress management training. The people in the control group were told to do none of these things. It’s hardly surprising that quitting smoking, exercising, reducing stress and dieting—when done together—improves heart health. But the fact that the participants were making all of these lifestyle changes means that we cannot make any inferences about the effect of the diet alone.
So when Ornish wrote in his op–ed that ‘for reversing disease, a whole-foods, plant-based diet seems to be necessary,’ he is incorrect. It’s possible that quitting smoking, exercising and stress management, without the dieting, would have had the same effect—but we don’t know; it’s also possible that his diet alone would not reverse heart disease symptoms. Again, we don’t know because his studies have not been designed in a way that can tell us anything about the effect of his diet alone. There’s also another issue to consider: Although Ornish emphasizes that his diet is low in fat and animal protein, it also eliminates refined carbohydrates. If his diet works—and again, we don’t know for sure that it does—is that because it reduces protein or fat or refined carbohydrates?”
I’m not paying a lot of attention to what Ornish says.
Exercise is more important than business
Why Exercising Is a Higher Priority Than My Business is an article in the Personal Health section of Entrepreneur magazine. The writer Joshua Steimle explains why he puts exercise above such things as client meetings. He says:
“I schedule my workouts during the workday and prioritize exercise over all my work activities. There is some flexibility, but if there is a conflict between a trail run I need to get in, and a meeting with a client, I’ll reschedule the client meeting first. I do this because I and my business can survive the consequences of rescheduling a client meeting, even if it means losing that client. But as soon as I start pushing workouts off, I’ll start missing workouts, and once I start missing workouts, I’m close to stopping workouts altogether.
Exercise must come first, or it’s unlikely to happen at all.
If exercise stops, then my health goes downhill. With the loss of physical health my productivity at work goes down. I become depressed. I lose motivation to do the things that makes my business successful. I’ve learned firsthand that excellence in one area of my life promotes excellence in all other areas of my life. Exercise is the easiest area of my life to control. It’s easy to measure. Either I get it in, or I don’t. When I do, it lifts up all other areas of my life, including my business.”
Smart man!
Avoiding pesticides in produce from Consumer Reports
To this point, I haven’t been fully convinced that organic produce is better for me. Though there’s a lot of fear-mongering and weird conspiracy theories around organic (and GMO) food, I haven’t found overwhelming evidence that organic produce is a) more nutritious or b) safer. An article in Consumer Reports has made me reconsider that stance.
“Experts at Consumer Reports believe that organic is always the best choice because it is better for your health, the environment, and the people who grow our food. The risk from pesticides on conventional produce varies from very low to very high, depending on the type of produce and on the country where it’s grown. The differences can be dramatic. For instance, eating one serving of green beans from the U.S. is 200 times riskier than eating a serving of U.S.-grown broccoli.”
The article provides an interactive guide so you can see where various fruits and vegetables lie on the spectrum from high- to low-risk:
“If you want to minimize your pesticide exposure, see our risk guide. (Download our full scientific report, ‘From Crop to Table.’) We’ve placed fruits and vegetables into five risk categories—from very low to very high. In many cases there’s a conventional item with a pesticide risk as low as organic. Below, you’ll find our experts’ answers to the most pressing questions about how pesticides affect health and the environment. Together, this information will help you make the best choices for you and your family.
This short video from Consumer Reports summarizes their findings.
Gaining a competitive edge
I’m a fan of Alex Hutchinson’s Sweat Science colum in Runner’s World. Hutchinson is a former physicist, an award-winning science journalist and a runner. (Check out his bio.) He always does a good job of discussing the research that’s available on any number of fitness and sports related topics from training methods to diet to whatever else you can think of.
Recently he wrote Advice to a Young Athlete. The article started as a response to a cyclist who wrote to him asking for advice on getting to the elite level. Hutchinson insists first and foremost that talent and hard work are the essentials. Beyond that there are a galaxy of things (supplements, training methods, etc) that may or may not work.
In this piece he discusses the following:
caffeine
acidity buffers: baking soda, sodium citrate and beta-alinine
My Achilles pain was getting better and then it flared up again recently and it has stayed flared for a while. This has been an ugly aggravation as it was a serious regression. Now, I’m very happy to report that my Achilles tendon irritation seems to be fading away. I’ve done three short-distance run/walks with no pain. (Will it stay gone is the real question.) What has helped?
Time off
Initially I thought that simply changing the way I ran would allow me to side-step whatever healing process that needed to take place. I revisited several technique changes that helped me overcome a past bout of Achilles pain. I discovered that there was no magic fix. Minding my technique is a good idea but it seems my tissues still needed time to heal.
Heel lift
I put a 1/4 inch heel lift in my shoe. The idea is to give a little bit of slack to the sore tendon.
To this point, I made sure not to do much in the way of stretching the tendon. It’s often a mistake to think that if it’s sore, it must need stretching. In fact, the damage to the Achilles may have been brought on by it’s being stretched too much and/or too fast.
I think this has been a BIG ONE. I believe that part of my problem stems from my inability to adequately anchor to the ground the distal end of my first metatarsal, aka the ball of my big toe. How might that affect my Achilles tendon?
Too much of this may over-stress the Achilles and cause pain.
If I can’t secure that first met head to the ground then I have a weak foot tripod as the Gait Guys have described it.That means that my foot might pronate in an uncontrolled way which can result in something like the image to the right. Too much of that done too often and/or too fast could over-stress the Achilles causing damage and pain. To form a solid foot tripod, I need to be able to secure the center of my calcaneus (heel bone), first metatarsal head (ball of the big toe) and the fifth metatarsal head (ball of the little toe.)
(To be clear, I can’t say this is The Cause for anyone else’s Achilles problems. Someone else may be able to run with lots of pronation and feel fine.)
How did I know I had difficulty getting that met head to the ground? I’ve been videoed running and I could see this extended pronation occurring. I could feel it as I tried doing the exercise in the following video. This gets into what seems like some real minutiae. For me, it seems pretty important. Also, I don’t believe this movement is trained in the eccentric strength protocol I mentioned above.
Metronome running
I’ve read several discussions (here, here, here) on running cadence and loading rate as it pertains to injury risk. Essentially, by using a quicker cadence we should load the tissues of the foot for less time per foot fall thus resulting in less stress to those tissues. That’s exactly something I need.
I went back to using a metronome when I run so that I can make sure to keep a quick pace. I set the metronome from 170 to 180 bpm and matched my cadence to the beat. It’s definitely a quicker cadence than what I’m used to. Seems I’ve backslid some on minding my cadence. Going forward, I think it will be a good idea to periodically run with a metronome to ensure that I’m staying quick on my feet.
About three weeks ago I went for a run in the snow. Part way through I felt some irritation in my left Achilles tendon. Like anyone who loves/needs to exercise, I kept running and I tried to convince myself that it wasn’t too bad, that it would probably go away soon or maybe if I changed my stride slightly it would resolve during the run.
I was wrong! I really irritated the thing and had to walk about a mile. This was the latest flare-up of a years-long lingering issue. (I’ve discussed the Achilles here and here, as well as left heel pain/plantar fasciitis here, here, here, here, here and probably in some other places… You’d think for someone who’s considered this issue so much that I wouldn’t have it anymore.)
Prior to this Achilles flare-up, I’d had some of some old familiar heel pain. It wasn’t debilitating but it was a signal that something wasn’t as it should be. Again, I ignored it to a large degree and figured it would resolve. I should’ve paid closer attention to it. Essentially, it wasn’t a problem until it was a problem. Time to get back to work on this thing.
Tendon injury: A complex issue
Why do we get injured? How do our tissues (like tendons) become damaged? If we administer the right amount of stress and then recover we get a positive adaptation–we get stronger. In contrast, if we administer too much stress and we don’t recover then we get some type of injury. Thus too much stress delivered too often and/or too fast has been my problem. I need to increase my tissue tolerance to the forces of running.
A recent article from Alex Hutchinson is titled Pro Tips on Treating Tendon Injuries. This article covers a debate among members of the Canadian Association of Sports and Exercise Medicine in Ottawa. Several top sports physicians and therapists were asked: Which therapy should the squash player try next? (I’m not a squash player but I have the injury they discussed.) If you’re dealing with this issue it’s definitely worth a read. It discusses several methods: eccentric strengthening, nitroglycerin patch, dry needling, cortisone, and platelet-rich plasma.
There wasn’t 100% agreement on anything much, but Hutchinson’s concluding statement was this (emphasis is mine):
“So what should the poor squash player do? In the question period following the debate, most participants conceded that strengthening exercises are the path to long-term health. Depending on the specifics of your tendon injury, other techniques may provide relief to allow you to exercise, but they’re not permanent cures.”
Cures I like. I have no interest in simply treating symptoms. Thus I decided it was time to implement something with which I’d been familiar but which I knew wouldn’t be very exciting at all: the eccentric strength protocol.
Eccentric strengthening
First, what does “eccentric” mean?An eccentric contraction is one in which the muscle is contracted but it’s also lengthening. Think of doing a bicep curl. You know the part where you yield to gravity and lower the weight? That’s the eccentric portion of the movement. (In contrast, the concentric portion is where you overcome gravity and bring up the weight.) For this particular protocol, we want to fight against the lowering action and lower very slowly.
The strength protocol consists of two exercises: a straight-kneed and a bent-kneed eccentric heel drop. The protocol calls for three sets of fifteen heel drops, both bent- kneed and straight-kneed, twice a day for twelve weeks.
Standing on a step with your ankles plantarflexed (at the top of a “calf raise”), shift all of your weight onto the injured leg. Slowly use your calf muscles to lower your body down, dropping your heel beneath your forefoot. Use your uninjured leg to return to the “up” position. Do not use the injured side to get back to the “up” position! The exercise is designed to cause some pain, and you are encouraged to continue doing it even with moderate discomfort. You should stop if the pain is excruciating, however.
Once you are able to do the heel drops without any pain, progressively add weight using a backpack. If you are unlucky enough to have Achilles tendon problems on both sides, use a step to help you get back to the “up” position, using your quads instead of your calves to return up.
The eccentric exercises are thought to selectively damage the Achilles tendon, stripping away the misaligned tendon fibers and allowing the body to lay down new fibers that are closer in alignment to the healthy collagen in the tendon. This is why moderate pain during the exercises is a good thing, and why adding weight over time is necessary to progressively strengthen the tendon.
You do these exercises for 3 sets of 15 reps, twice daily. There are photos showing these exercises including a modification if you have what’s known as insertional Achilles tendonitis. Again, read the whole thing if you want the full rundown of this protocol.
More thoughts
Part of why I haven’t done this in the past is that it is slow and tedious! Three sets of 15 slow reps makes time crawl like some sort of crippled tortoise. It ain’t fun! Plus I’ve never cared much for doing calf work. That said, I need to fix this problem. This process seems to be the best way to go about it, so I’m on board.
Something else I realize is that if I’m prone to this injury and I want to avoid it then I need to do the preventive work. That means setting aside time throughout the week and during my workouts to do some of this stuff.
I’ve been doing this work for about the past three weeks and I am getting better. I’ve done a couple of short run/walks and I’m not in the clear just yet. The only option I see is to continue doing what I’m doing.
Update
I just went on a run of a little over two miles and the Achilles feels fantastic. No pain! Felt like I could’ve run all day–which would’ve been stupid of me. This protocol is working for me right now.
Ever hear anyone exclaim with enthusiasm “Today is feet day!!” right before their workout? I haven’t. No one is very excited about working their feet. I’ll wager most of us don’t ever consider our feet until there’s some sort of pain or problem down there. The thing is, it’s only every single step of every single day that we might need our feet work well for us. As long as we live on a planet with gravity and we don’t want to walk on our hands, then we might want to consider whether or not our feet are doing the job they should be doing.
If when we walk, run, or step and our feet aren’t working well, then it’s very likely that something upstream from the feet may be compromised too. It’s analogous to a house built on a bad foundation. Lazy or immobile feet might affect the ankle which might affect the knee which might affect the hip, the back, the spine, the shoulders…
I’ve noticed improvement in a long-standing big toe issue by doing some of this work. I’ve also found some of these exercises very challenging as have several of my clients. Some of these drill may seem impossible at first but I and others have found that with a bit of mindful work, we can get these foot muscles to work in a few days to a week. It does take some focused work but maybe just a few minutes a day.
Moving and using our sore parts–confronting the pain–is essential to getting rid of pain.
The writer discusses his journey following a bike crash which hurt his knee (an acute injury). He rested and took pain medicine. He states (emphasis is mine):
“It turns out my belly-up approach was dated. New research is proving that the best way to treat nagging pain is to eschew pampering in favor of tough love. Doctors at the University of Pittsburgh are doing ongoing research showing that stretching irritated tendons actually reduces inflammation. And the principle extends beyond rickety wiring. Every expert I spoke with told me variations of the same thing: ‘Rest and ibuprofen cure few injuries,‘ said Dr. Jeanne Doperak, a sports-medicine physician at the University of Pittsburgh. ‘During rest you’re in a non-healing zone,‘ offered Dr. Phelps Kip, an orthopedic surgeon and U.S. Ski Team physician. ‘The body was designed to move.'”
Pain is very much a psychological thing. I can relate to this:
“And it just so happens that tendinopathy chronic tendinitis is the most diabolical of recurring injuries. Give me a broken foot over tendon trouble any day when something snaps, at least you know what you’re in for. My injury dragged on into winter, deep-sixing my mood. This is not uncommon: The link between pain and depression is so well established that sports psychologists use a tool called a Profile of Mood States to monitor injured athletes. (This is a graph evaluating tension, depression, anger, vigor, fatigue, and confusion. People in pain score extremely high in every category except for vigor.) I was five years removed from being a college athlete and I was Long John Silvering it up stairs at work. Strange questions crept into my head: Could I consider gardening exercise?”
I like the overall message of the article but I don’t agree with all the information:
The writer says, “… or imbalances in the body’s kinetic chain of movement (a weak core can cause lower-back pain).”
Though this is a popular concept, there is significant evidence that “core strength” (which can be defined and measured in a multitude of ways) has nearly nothing to do with back pain.
For runner’s knee, the writer suggests this: “Lie sideways on a table, legs straight, and slowly raise and lower the upper leg ten times. Do three sets. Easy? Ask your PT for a light ankle weight.”
I think this might be part of an effective strategy to address runner’s knee (if the problem is rooted in the hip which it often is; however it could be rooted in poor control of the foot and ankle), but there are several dots that I think need connecting between this exercise and full-on running. This exercise is very different from running in which the foot impacts the ground and the runner must control motion at the foot, ankle, knee and hip. If this is the only exercise given to a runner’s knee patient then I’m skeptical that the runner will fully overcome the issue.
A caption under a photo reads, “Preventive Measures: Recovering from a nagging injury? Next time you go for a run or a ride, try taking ibuprofen beforehand. As long as you’re cleared for activity by your doctor, inhibiting swelling prior to a workout can dramatically reduce post-exercise inflammation and pain.”
This is an interesting idea but I have strong reservations. Pain is a signal that should be respected. Even though pain doesn’t equal injury it’s still a message from our brain that there is a perceived threat that needs to be addressed. The pain could be signaling a threat related to poor movement control and tissue stress is leading toward injury. By taking a pain-blocking drug, we might simply be turning down that signal as we continue with what may turn into an acute injury. I would compare this to driving a car with a damaged muffler that needs replacing and instead of replacing the muffler, we turn up the stereo loud: No noise!!–but have we fixed the problem?
On the other hand, I understand that even if the movement problem is addressed, we may still feel pain. Taking a drug may help the brain experience the new, better movement in a painless way which might help break the chronic pain cycle. I’m curious to what degree this has been method has been investigated.
For me, as a personal trainer, I would never suggest someone take a drug and just keep going. Rather, I would speak with the person’s PT. If he or she OKs it, I would then advise someone to move and work below the pain threshold or at a very manageable level of pain.
I just found a fascinating video that speaks very much to some of the things I’ve been reading lately (and have read about in the past.) It’s an interview with a man named Stephen Jepson. In his former life he was a very accomplished ceramics maker and teacher (Is that what they’re called? Or potter?) He founded the World Pottery Institute and he even has a piece in the Smithsonian. Now his focus is Never Leave the Playground.
A grown-up at play
Jepson is in his 70s now and he literally spends his waking hours at play. He runs around, hops, crawls, juggles, rides a skateboard (and a variation thereof), elliptical bikes, and generally moves about the earth in very novel, random, playful ways. He’s not only having fun and staying fit, he’s also stimulating his brain in powerfully healthy ways according to research. More on that in a moment. Here’s the video:
Jepson says that his play improves such brain skills as cognition and memory. He seems to be very spot-on according to several things I’ve been reading.
“In the contest of movement, play can be thought of as a safeguard against habitually using the same movement pattern to solve a particular motor challenge and ignoring potentially better solutions.
Thus we can look at our motivation to play as a natural incentive to experiment with new solutions, even if they don’t appear superior at first glance. We could also look at play as a way to ‘return to the drawing board’ or start over from scratch on a movement problem without preconceived notions about the right or wrong way to move.”
What this says to me is that novel, unusual movement gives us the opportunity to build a broad movement database or maybe a movement Swiss Army knife. We add to our available movement repertoire when we move in as many ways as possible in as many environments as possible: rolling on the ground, climbing, crawling, standing on different surfaces, moving at all speeds, lunging in many directions. Perhaps as a result, when confronted with a movement scenario that’s a little out of the ordinary our brain may say, “Oh, I’ve been here before. I have multiple strategies for moving safely and effectively here.”
The science of play & the brain
In his book, Hargrove references a NY Times article titled Taking Play Seriously. It states:
“For all its variety, however, there is something common to play in all its protean forms: variety itself. The essence of play is that the sequence of actions is fluid and scattered. In the words of Marc Bekoff, an evolutionary biologist at the University of Colorado, play is at its core ‘’a behavioral kaleidoscope.’”
‘I think of play as training for the unexpected,’ Bekoff says. ‘Behavioral flexibility and variability is adaptive; in animals it’s really important to be able to change your behavior in a changing environment.’ Play, he says, ‘leads to mental suppleness and a broader behavioral vocabulary, which in turn helps the animal achieve success in the ways that matter: group dominance, mate selection, avoiding capture and finding food.”
This flexibility and growth potential of the brain is known as neuroplasticity. Though Stephen Jepson doesn’t use that word in his interview, he’s talking all about neurplasticity as he describes the benefits to his brain and both vigorous physical activity and play. His thoughts are supported by research:
Neuroscience and Biobehavioral Reviews,Beneficial effects of physical exercise on neuroplasticity and cognition: “The results suggest that physical exercise may trigger processes facilitating neuroplasticity and, thereby, enhances an individual’s capacity to respond to new demands with behavioral adaptations. Indeed, some recent studies have suggested that combining physical and cognitive training might result in a mutual enhancement of both interventions.”
Archives of Medical Research, Physical activity, brain plasticity, and Alzheimer’s disease: “We conclude from this review that there is convincing evidence that physical activity has a consistent and robust association with brain regions implicated in age-related cognitive decline and Alzheimer’s disease. “
The Importance of Play, Dr. David Whitebread, University of Cambridge: “For example, playful rats have been shown to have significantly elevated levels of brain-derived neurotrophic factor (BDNF), which is recognised to have a central role in developing and maintaining neural plasticity (or, the ability to learn). They have also demonstrated that play supports novel neural connections and changes the architectural structure of significant brain regions. Play deprived rats became more aggressive to other rats, were less able to mate successfully, and showed heightened levels of fear and uncertainty in novel environments.” (To be clear, this is a rat study but similarities have been seen in observation of humans.)
Inside my brain
All of this is enormously fascinating and inspiring to me. It has me thinking a lot about my own fitness process as well as that of my clients. I’ve been doing a little indoor rock climbing lately and that’s a completely different type of workout. I’ve also done a little bit of cross-country skiing and I hope to take a lesson and increase my skill there. I look forward to trail running and mountain biking soon. I find both activities highly engaging, and both offer endless opportunities to negotiate with gravity in myriad different ways.
I’ve discussed my recent experience with the FASTER Global course this summer (Part I, Part II, Part III, Part IV). As a result, my eyes (and brain) have been opened very wide to almost infinite opportunities for innovative, play-like movement strategies.
My hope is that my clients are having some degree of fun already but now I’m thinking much more about injecting an aspect of play into our sessions. Lots to think about…